Medicaid Overview
Medicaid is a critical source of health care coverage for children and youth with special health care needs (CYSHCN). In fact, it is the single largest payer in the U.S. for children, including CYSHCN. State Title V programs are statutorily required to collaborate with Medicaid in different ways. Being equipped with knowledge of the state Medicaid program allows Title V staff to engage as well-informed partners, identify opportunities for partnership, and draw on their expertise to provide tailored input to Medicaid partners.
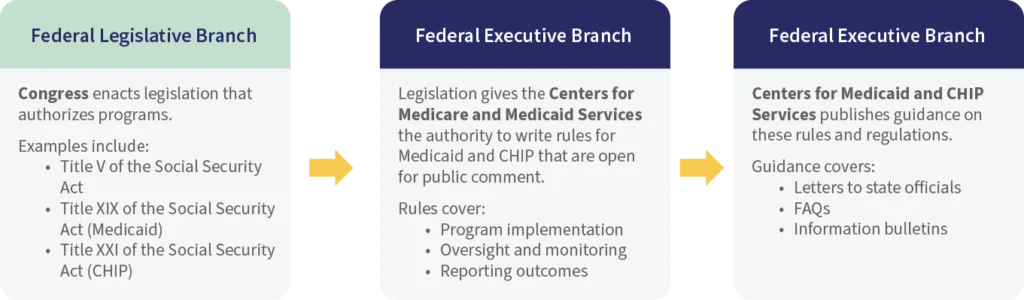
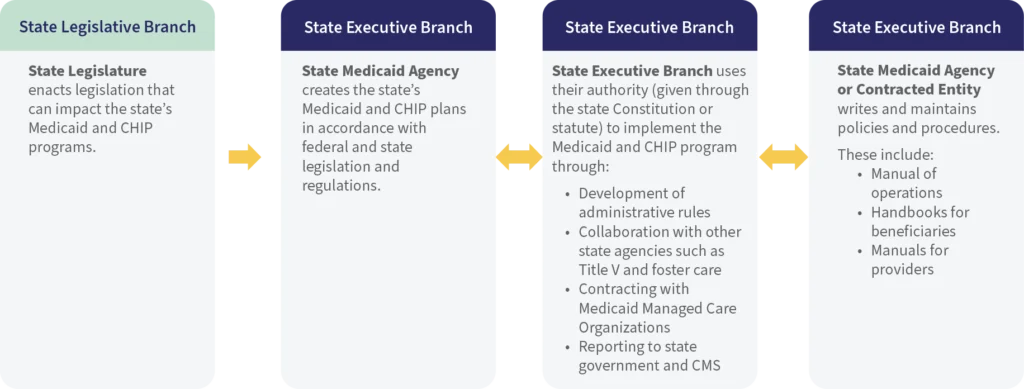
Roles of the Federal and State Government in Medicaid
Medicaid was established in 1965 in Title XIX of the Social Security Act, which also established Medicare. It was originally designed to increase access to health care for low-income individuals. This section of the workbook breaks down the roles of the federal and state legislative and executive branches and their role in Medicaid.
| Federal Government | State Government | |
|---|---|---|
|
Administration |
|
|
|
Financing |
|
|
|
Program Rules and Regulations |
|
|
*Note: See the Medicaid Benefits Section for more information on cost sharing in Medicaid.
Pathways to Medicaid Coverage for CYSHCN
By Income, Not Health Status
States establish income eligibility criteria either as a dollar threshold or as a percentage of the Federal Poverty Level (FPL). States have flexibility in establishing income-based eligibility, as long as it is not lower than the federal limit of 138% FPL. The FPL is updated every year, and it is adjusted to account for inflation.
By Income and Functional Disability
Individuals who are eligible for Supplemental Security Income (SSI) are eligible for Medicaid in most states. Eligibility for SSI is based on income and meeting the Social Security Administration’s definition of disability. In many states, individuals who receive SSI are eligible for Medicaid. However, in a few states, Medicaid eligibility is not aligned with eligibility for SSI. These states are known as “209(b) states.”
By Severe Disability (TEFRA State Plan Option and Home- and Community-Based Service Waiver Programs)
States may choose to implement programs that allow them to enroll CYSHCN who require an institutional level of care in Medicaid regardless of family income. Each state can establish its own definition, but generally “institution level of care” means that a child needs a level of care that is typically provided in an institutional setting.
Foster Care
Children in foster care are eligible for Medicaid regardless of disability status or income level.

Medicaid Program Structure
Medicaid programs are funded jointly by the state and federal government. The federal government pays states a percentage of Medicaid program expenditures. This percentage is called the Federal Medical Assistance Percentage, or FMAP. The FMAP is a statutory formula that is updated at the federal level each year. The FMAP for a state is calculated based on the state’s per capita income. By law, the FMAP for a state cannot be lower than 50%. States with lower per capita income will have a higher FMAP.
The Medicaid state plan describes what services are covered for all Medicaid enrollees. Within the state plan, mandated benefits are those required by federal law in a state Medicaid plan. Optional benefits are services that state Medicaid programs can choose to cover but are not required by federal law.

How do States Make Changes to their Medicaid Programs?
State Medicaid agencies have two primary mechanisms for making changes to their Medicaid programs: state plan amendments (SPAs) and waivers. When a state would like to make a change to its Medicaid program and policies, it will submit a state plan amendment to CMS for review and approval. States must submit a SPA even if the change in the program is permitted by federal laws and rules. Medicaid waivers are state requests to CMS to ask for permission to “waive” certain requirements of the Social Security Act. Two main types of significance to CYSHCN are 1115 demonstration waivers and 1915(c) Home-and Community-Based Services waivers. To learn more about waivers, go to the workbook section on TEFRA and Home- and Community-Based Services (HCBS) Waivers.
Federal Laws and regulations specify that state Medicaid programs must include certain benefits such as Early, Periodic Screening, Diagnostic, and Treatment (EPSDT) benefits. However, states have the option to charge premiums and to establish cost sharing requirements for Medicaid enrollees. For more information, go to the EPSDT workbook chapter.
State Plan Options Under Medicaid
Affordable Care Act
The Affordable Care Act of 2010 originally required states to expand Medicaid eligibility to all adults with incomes up to 138% FPL. After this policy was contested in the courts, the policy became optional for states. While the Medicaid expansion policy applies only to adults, research has established a parental “welcome mat” effect in which health coverage among children already eligible for Medicaid or CHIP increases when their parents become eligible as well.
Use this resource from the Kaiser Family Foundation to see what states have expanded Medicaid:
Family Opportunity Act
The Family Opportunity Act (FOA) was passed as part of the Deficit Reduction Act in 2005. It offers states the opportunity to create a buy-in program to extend Medicaid coverage to children who meet SSI disability criteria, but whose family incomes are too high to be eligible for SSI. Family incomes must still fall below 300% FPL for them to be eligible. Under this option, state Medicaid programs are allowed to charge premiums to families whose children with disabilities are enrolled in Medicaid through the FOA. A buy-in program allows both uninsured and underinsured children to be eligible to enroll in Medicaid. Medicaid, especially the EPSDT benefit, can play a crucial role in filling gaps in coverage for CYSHCN covered by commercial insurance. See the EPSDT workbook section for more information on children with a combination of Medicaid and private insurance.
TEFRA
This state plan option is named for the legislation that contains it, the Tax Equity and Fiscal Responsibility Act (TEFRA) of 1982. As described above in the Pathways to Medicaid section, this state plan option allows state Medicaid programs to extend Medicaid eligibility to children who require an “institutional level of care.” Read more in the TEFRA section of the workbook.
Health Homes
Health Homes provide a system of comprehensive care coordination to Medicaid beneficiaries who have chronic conditions. States are allowed to determine health home provider eligibility, and some states use this discretion to design health homes that specifically serve CYSHCN. Examples include children with medical complexity (CMC) served by pediatric specialists, or children with serious mental illness served by behavioral health providers. Another Health Home option for states was established by the Advancing Care for Exceptional (ACE) Kids Act in 2019. The ACE Kids Act allows states to develop health homes targeted to children with medical complexity.
Reimbursement for Expanded School-based Health Services
In 1997, CMS implemented what was known as the “Free Care Rule” which limited the ability of education systems to bill Medicaid for student health care services. CMS reversed this policy in 2014, creating an opportunity for state education systems to expand reimbursement for school-based health services provided to Medicaid beneficiaries, including CYSHCN.


Learn More About the Title V and
Medicaid Partnership
Tools, Templates, and Tips
Medicaid and CHIP Payment and Access Commission (MACPAC)
Annotated Title XIX and Title XXI
https://www.macpac.gov/publication/annotated-statutes-for-medicaid-and-chip/
Reference Guide to Federal Medicaid Laws and Regulations
